Pneumothorax means the intrusion of air into the pleural cavity of the chest. It leads to the collapse of the lungs and impaired breathing. Why does pneumothorax occur and how does it manifest itself? How to give first aid?
Pneumothorax occurs when air enters the pleural cavity of the chest. The accumulated and increased air pressure causes the lungs to collapse and impairs breathing and circulation.
In most cases, it is a life-threatening condition. Types and kinds of pneumothorax, first symptoms, quick help, treatment and many other interesting information can be found in the article.
What is pneumothorax and pleural cavity?
The lungs of a person are located in the rib cage. Their surface is covered with a thin covering (membrane) called the pleura - pleura. A similar membrane is also located on the inside of the chest and is called the pleura.
Between these two thoracic membranes is a space professionally called the pleural cavity.
The pleural cavity is filled with a small amount of a special fluid. The fluid serves to keep the diaphragms moving and shifting during breathing (respiration). Thus, the role of the pleural cavity is to protect the lungs from the chest wall.
Under physiological conditions, the pleural cavity is under negative pressure. Both the right and left lungs have their own pleural cavity.
Pneumothorax occurs when air enters the pleural cavity. The accumulation of air in this space, between the chest wall and the lungs, causes excessive pressure on the lungs. The lungs subsequently collapse and shrink.
Pneumothorax is a life-threatening condition.
Causes
The etiology of pneumothorax varies. This condition can arise spontaneously in association with another more serious disease. However, most often it arises after trauma and mechanical damage.
Pneumothorax is divided according to the type of damage into:
Open
It occurs when air from the external environment enters the pleural cavity after the chest wall is breached. In open pneumothorax, there is contact and exchange of air between the pleural cavity of the individual and the external environment.
Closed
Occurs when air from internal structures enters the pleural cavity, especially when there is injury and disruption of the lung environment. In a closed pneumothorax, there is no contact and exchange of air between the individual's pleural cavity and the external environment.
Pneumothorax is divided into several types according to the cause of its occurrence:
Traumatic
Spontaneous
Iatrogenic
Traumatic tension pneumothorax
Tension pneumothorax is the result of any injury to the chest wall. Tension pneumothorax carries a serious risk of lung collapse.
The valve mechanism allows free air to enter the pleural cavity without escaping.
It occurs when air enters the pleural cavity unidirectionally during inspiration. Thus, air accumulates in the cavity around the lung and oppression and shrinkage of the lung organ occurs.
As the pressure increases, the contents of the cavity are pushed to the other side. The opposite lung is compressed. As a result of the compression of the lung on the other side, hypoxia - lack of oxygen - occurs.
There is impaired vascular return of blood, circulation, decreased cardiac output and a drop in blood pressure.
Spontaneous pneumothorax
Spontaneous accumulation of air occurs when the pleura ruptures. Air from the lungs thus escapes into the pleural cavity.
This condition arises mainly in more serious diseases such as tuberculosis, COPD, cystic fibrosis, pulmonary emphysema, pulmonary abscess and other conditions in which there is a risk of air cavities.
With the disease and simultaneous vigorous movement, coughing or breathing, damage to the pleural cavity wall may occur.
Iatrogenic pneumothorax
Iatrogenic pneumothorax is also called artificial pneumothorax. It occurs after diagnostic or therapeutic intervention by a physician. It occurs mainly during invasive surgery in the thoracic region.
Examples include lung biopsy, venous catheter insertion, spinal puncture, acupuncture or pressure ventilation.
Other types of pneumothorax
In addition to air, various types of fluid may enter the pleural cavity. In a physiological state, 10 to 15 ml of fluid is found in the cavity. In pathological circumstances, the amount of fluid may increase to several litres.
These are mainly water, blood and lymph. When it accumulates in the pleural cavity, we technically speak of hydrothorax, when blood accumulates it is haemothorax and in the case of lymph leakage it is chylothorax.
The most common injuries leading to pneumothorax are car accidents, falling off a bicycle, broken ribs, severe blows to the chest, stab wounds to the chest, gunshot wounds and diving to great depths.
Collapse of the lung is more common in tall and thin patients. However, it can occur in patients of any age and stature.
Possible causes of pneumothorax:
Chest contusion and concussion
Penetrating mechanical trauma
Stab and gunshot injuries
Frontal and side impact
Bronchial lung biopsy
Central venous cannulation
Artificial pulmonary ventilation
In resuscitation and rib fractures
Tuberculosis of the lung
Obstructive pulmonary disease (COPD)
Bacterial pneumonia (infection)
Cystic fibrosis
Lung emphysema
Lung abscess
Bronchial asthma
Acupuncture
Spinal ulcer
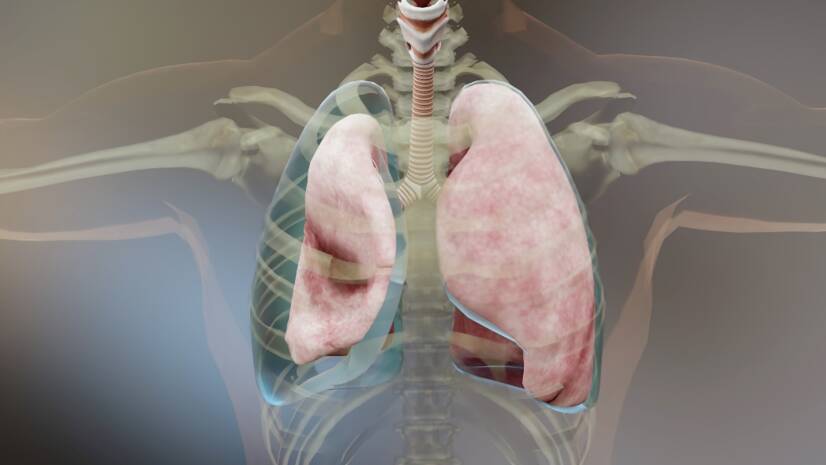
Pneumothorax: healthy and collapsed lungs. Trachea (larynx), pleural space (pleural cavity), air in the pleural space (accumulated air in the pleural cavity of the chest). Source: Getty Images
Symptoms
Severity of symptomsis related to the cause of the onset and the amount of air that enters the pleuracavity.
If the volume of air continues to increase, it can adversely affect the function of the heart and cause a life-threatening condition.
Trauma and mechanical injuries are common causes of lung collapse. Pneumothorax is manifested by other clinical signs, such as severe chest pain that is sudden and rather stabbing and sharp.
Excessive dyspnoea, discomfort in breathing and a feeling of shortness of breath are present. An irritating cough is also common.
Associated symptoms, such as pallor of the skin, blueness of the mucous membranes and lips (cyanosis), a decrease in blood pressure and, conversely, an increase in heart rate, are associated with the subsequent pathological breathing and inadequate oxygenation of the body.
Associated symptoms and manifestations of pneumothorax:
Sudden chest pain
Feeling of lack of air
Severe shortness of breath
Dry irritating cough
Rapid shallow breathing
Pallor of the skin
Blue discoloration of mucous membranes and lips (cyanosis)
First aid for pneumothorax: How to proceed correctly?
If you are in the vicinity of an individual who has an open chest injury, this is a life-threatening condition. The affected person should be given immediate first aid.
However, in this case, it is not a case of conventional first aid.
First of all, it is important to assess the condition of the injured person and his breathing capacity. It is important to recognise the typical symptoms of pneumothorax, such as shortness of breath, shallow breathing, pallor of the skin, blueness of the mucous membranes and shock. It is necessary to call the emergency medical services immediately.
Pneumothorax often occurs as a result of injury to the chest cavity. It is therefore easy to find blood oozing out of the chest, which is bright red and foamy at the wound. If there is a foreign object in the chest, it is advisable not to remove it and to wait for professional help (unless a specialist tells you otherwise over the phone).
Place the injured person in a semi-sitting position and try to avoid unnecessary movements of the patient. It is advisable that the injured person tries to calm down and puts his upper limbs on some support (ground).
The open wound should be semi-closed to prevent excessive air from entering the pleural cavity. Ideally, a semi-permeable dressing should be made, consisting of an inner sterile layer followed by an impermeable layer - for example, a plastic sheet. The underside of the dressing is not fixed for blood drainage.
However, for the lay public, it is quite difficult to make a properly functioning semi-permeable dressing. Therefore, the new standards do not recommend making an impermeable dressing. Some sources, on the other hand, recommend leaving the dressing open on the wound.
Keep the injured person warm by covering them with a blanket or sitting on a blanket. The goal is to isolate the heat.
Monitor the casualty's condition until the ambulance arrives. If the casualty stops breathing, start CPR.
Continuous contact with the rescue caller is appropriate until the arrival of the rescue service itself. In case of doubt, direct consultation with a specialist is possible.
Diagnostics
In acute traumatic pneumothorax, the patient is given first aid and is taken by ambulance to the operating room. The diagnostic process is accelerated in this case.
An important role is played by the ambulance service, which is summoned to most traumatic chest cases. Diagnosis begins at the moment of arrival of the first aid.
Diagnosis (especially for closed pnenumothorax) is usually made by taking a history, assessing clinical symptoms and basic physical examination (tapping, listening and palpation).
Pneumothorax is a relatively straightforward diagnosis for the specialist. Thus, basic information on clinical symptoms, physical examination and imaging (most commonly X-ray) is sufficient.
However, ECG (electrocardiography), CT (computed tomography), blood gas examination or thoracoscopy (endoscopic examination of the pleural cavity) may be indicated.
In a hospital setting, the diagnosis is confirmed by a chest X-ray. The image clearly shows collapsed, shrunken lungs surrounded by air. In the most severe cases, the heart may also be seen displaced towards the healthy side of the lungs.
X-ray - pneumothorax of the left lung and accumulation of air in the pleural cavity of the chest (white colour). Source: Getty Images
Prevention of pneumothorax
There is no prevention of pneumothorax as such. However, it is possible to eliminate certain risk factors leading to its occurrence.
The key to prevention is professional treatment of the underlying disease. Adherence to lifestyle principles and drug therapy in the diagnosis of various diseases such as COPD, bronchial asthma, pneumonia, bronchitis, tuberculosis and others.
Early professional treatment of any respiratory tract infection and not delaying a visit to the doctor is advisable.
In particular, regular adequate exercise, avoidance of tobacco products, adherence to anti-allergy measures and sufficient exposure to fresh, healthy air are basic preventive measures for respiratory health.
Prevention also involves eliminating the risk of injury and mechanical damage to the chest during risky activities. Examples include wearing seat belts in the car, obeying traffic laws and avoiding jumping and diving into deep water.
Patients who have had a pneumothorax should avoid excessive physical exertion and pressure on the lungs. They should follow lifestyle guidelines to prevent recurrence of the disease.
Principles for individuals after overcoming pneumothorax:
If you experience sudden chest pain and shortness of breath, call emergency services immediately.
Avoid excessively heavy physical activity.
Avoid excessive pressure on the chest/lungs.
Avoid air travel for one year after having a pneumothorax.
Avoid diving to great depths.
Avoid smoking tobacco products.
See a pneumologist regularly as a preventive measure.
How it is treated: Pneumothorax
Treatment of pneumothorax: Medication, puncture or surgery
VODIČKA, Josef. Traumatology of the chest. Prague: ISBN 978-80-7492-168-1.
HYTYCH, Vladislav and Alice TAŠKOVÁ. Traumatology of the chest in instructive case reports. Prague: Institute for Public Health Care: Maxdorf, [2017]. Jessenius. ISBN 978-80-7345-526-2
healthline.com - Pneumothorax (lung collapse). healthline. by Lydia Krause
internimedicina.com - A brief introduction to acute pneumology. Pavel Turčani, MD
medicalnewstoday.com - What to know about pneumothorax. Medical News Today. Jon Johnson
I completed my bachelor's degree in physiotherapy at the Faculty of Biomedical Engineering of the Czech Technical University in Prague. I continued and completed my master's degree in physiotherapy at the Faculty of Health Engineering of TnUAD. I am currently pursuing my PhD rigorosis at the Slovak University of Health Sciences in Bratislava. During my studies I worked as a physiotherapist in the rehabilitation clinic of Vamed Mediterra in Prague and then as a physiotherapist at the Regional Hospital in Liberec in the Department of Neurology. During my employment I was part of the medical team in the Covid19 department. I am mostly interested in human musculoskeletal system, rehabilitation, physiotherapy in gynaecology and natural medicine. My hobbies include exercising, running, writing and managing social media.
, pleural space (pleural cavity), air in the pleural space (accumulated air in the pleural cavity of the chest). Source: Getty Images")
. Source: Getty Images")










