Cervical cancer is a disease that can be caught during regular gynaecological examinations by screening, which is carried out once a year in the gynaecologist's office. When caught early, it is one of the most successfully treatable cancers.
Cervical cancer is a cancer arising from the cervix.
Cervical cancer is the fourth most common cancer in women, most often affecting younger women under the age of 45.
With regular gynecological check-ups, it is easily diagnosed at an early stage with effective treatment.
Anatomy of the female reproductive organ
The internal reproductive organs consist of:
Cervix - it is cylindrical in shape at the end of the uterus and forms a canal between the uterus and the vagina. The outer portal of the cervix is covered with mucus, which prevents bacteria from entering the uterus.
Vagina – The vagina connects the internal genital organs to the external ones. It is about 7-10 cm long, elastic and lengthens during sexual intercourse.
Maternica - It is a hollow organ, located in the small pelvis and consisting of the body of the uterus, and the cervix.
Fallopian tubes - The fallopian tubes are located in the upper part of the uterus. They are thin tubes about 1 cm thick and 10-12 cm long. Their job is to catch the egg released from the ovary during ongoing ovulation.
Ovaries - They produce female sex hormones and secrete an egg ready for fertilization during ovulation.
Cervical cancer begins to form in the tissues of the cervix by the formation of abnormal cells. Its formation is most often related to HPV infection, which has been detected in 99% of cervical cancers.
It is usually a slow-growing cancer that may be asymptomatic and is picked up in a preventive screening examination.
Cervical cancer is most common in developing countries with lower rates of prevention
The disease can have varying degrees of severity, with uterine varicocele affecting several types of tumours.
Types of cervical cancer
Squamous cell tumours account for 70-80% of cervical cancers. This type of cancer starts in the thin, flat cells lining the cervix.
Glandular tumours, or adenocarcinoma, account for 20-25% of cervical cancers. Their formation begins in the mucus- and other fluid-producing cells of the neck.
Other epithelial tumors are rarer.
Classification according to advanced disease
The term cervical intraepithelial neoplasia (CIN) is used to describe a change in the cervix that is not yet cancerous but may lead to cancer over time.
It is classified into three stages
CIN 1 – Abnormal cells are found at one-third of the thickness of the cervical layer. These changes may return to normal with time and in most cases no treatment is needed.
CIN 2 - Abnormal cells are found in one to two-thirds of the thickness of the neck layer.
CIN 3 – Abnormal cells cover the entire thickness of the cervical layer.
In CIN 2 and CIN 3, abnormal cells are removed to prevent cancer from developing over time.
According to the FIGO staging system, 4 stages of cancer are determined. The lower the number, the better the prognosis.
Along with the FIGO system, the TNM system is used to determine the stage of cervical cancer ( T - tumour, size of the tumour, N - nodes, whether the tumour has spread to the lymph nodes, and M - metastasis, spread to distant sites in the body).
FIGO stages
Stage 1 - The tumor is located only on the cervix.
Stage 2 - The tumor is already affecting tissues outside the uterus, but it does not go into the pelvic wall or the lower part of the vagina.
Stage 3 - The tumor also affects the lower third of the vagina, the pelvic wall, or causes damage and dysfunction of the kidney.
Stage 4 - The tumor has spread to the pelvis, extending into the bladder or rectum. The cancer has spread to distant organs outside the pelvis, affecting the lymphatic system and metastasizing to the lungs, bones, or liver.
Causes
HPV infection is an etiologic factor of the cause of cervical cancer.
However, HPV infection alone, i.e. human papillomavirus, cannot cause cancer. Other factors besides HPV infection are required for the development of cancer and for its tumour growth and malignant progression.
Transmission of HPV infection is possible through a variety of routes, but the most important is through sexual contact and therefore occurs mainly in sexually active people.
Most types of HPV do not cause any problems and go away on their own. Some types cause genital warts, for example, and some cause changes to the cervix, leading to the development of cervical cancer.
Risk factors that increase the development of cervical cancer are:
Previous cancers of the vagina, vulva, pelvis, urinary tract.
Having no risk factors doesn't mean you won't get cervical cancer for sure
Factors that reduce the development of cancer:
Safe sex
Vaccination against HPV virus
Regular screening to detect abnormal changes on the cervix
Prevention
Cervical cancer can be monitored withregular check-ups.
HPV vaccines are now also available to protect against cervical cancer as well as other HPV-related diseases.
HPV vaccination
Vaccination against human papillomavirus (HPV) is one of the most important prevention programmes.
Some HPV vaccines:
Cervarix, protects against 2 types of HPV
Gardasil, protects against 4 types of HPV
Gardasil9, protects against 9 types of HPV
Girls, women, boys and men can be vaccinated.
The vaccine given before first sexual intercourse is most effective. A sexually active person administering the vaccine can significantly reduce the risk of developing disease from the HPV virus.
In the beginning, until the cells start to grow and the cancer starts, a woman does not experience any symptoms and it can most likely only be detected after a screening examination by a gynaecologist.
The most common symptoms of cervical cancer are:
bleeding between menstrual cycles.
discomfort, discomfort, pain during sexual intercourse.
bleeding after sexual intercourse, after exercise.
bleeding in postmenopausal women.
vaginal discharge with a strong odor.
vaginal discharge stained with blood.
pain in the pelvic area.
enlarged lymph nodes.
If the disease is not caught in time and the tumour spreads to the surrounding tissues, there is pain in the pelvis and sacrum, pain, burning when urinating, and later there is also weight loss, a decrease in overall physical performance, and there may even be so-called water in the abdomen, i.e. fluid in the area of the abdominal wall.
Excessive enlargement of the lymph nodes can sometimes be manifested by unilateral swelling of the limb.
Diagnostics
Currently, prebioptic methods are used for diagnosis. During regular prophylaxis with a gynaecologist, the pre-invasive stages of the disease are still caught.
In many European countries, every woman is entitled to free cervical cancer screening once a year as part of preventive gynaecological check-ups.
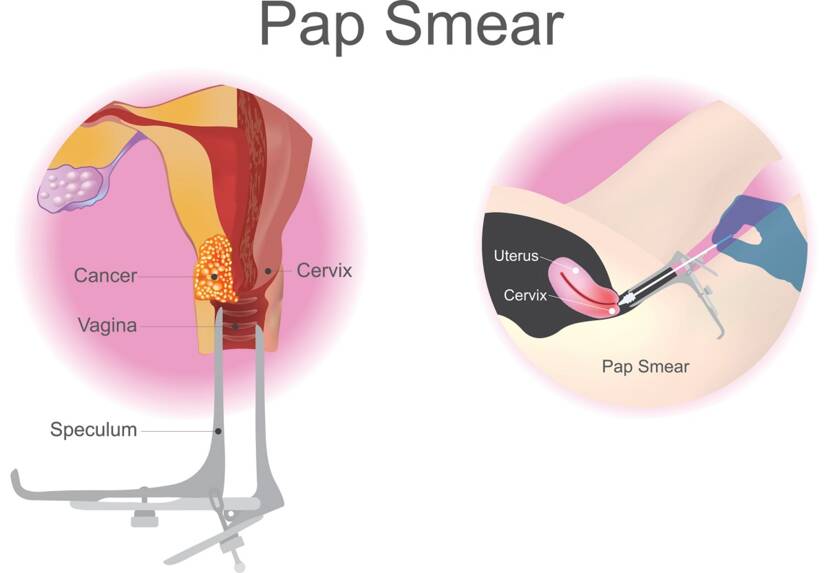
At the gynecological examination, a physical examination and an oncocytological smear of the cervix are performed.
Cervical cancer screening, a painless oncocytology smear of the cervix using a brush. (cervical pap smear, cervix, uterus, vaginal forceps). Photo: Getty Images.
Until recently, a Pap test was performed to detect changes in the cervix, which picked up abnormalities in the cells and reduced the incidence of cancer by 60-90%. Nowadays, the HPV DNA test is already in place, which has a higher sensitivity than the Pap test and provides greater protection against cervical cancer through early detection.
Diagnosis is done by examining the cervix, vagina and pelvis to detect abnormalities.
When abnormal cells are detected in the screening test, colposcopy is usually performed afterwards. Colposcopy allows a magnifying glass to be used to view the lump in detail. During the examination, a biopsy is taken: a tissue sample from the cervix.
Cone biopsy. During general anaesthesia, a cone-shaped piece of cervical tissue is taken and then the tissue is checked under a microscope to see if the sample contains cancer cells.
A biopsy is the extraction of sample cells or tissues for examination to determine the presence or extent of a disease. Source: Getty Images.
Based on the size of the tumour and lymph node involvement, the stage of the carcinoma is determined.
Determining the stage of the disease determines the extent, site of involvement and its spread to the surrounding area, also referred to as staging, a staging system called FIGO to determine the size of the tumor, its spread and any metastases present.
Staging of cervical cancer also requires other tests.
The examination is performed under general anaesthesia, when the woman is slightly anaesthetised and does not feel any pain, and the cervix, vagina and uterus, bladder, rectum are examined in detail and possible enlargement outside the cervix is detected. A tissue sample is taken from the abnormal cells, biopsied to check for cancer cells.
X-ray - chest x-ray to check the lungs and chest cavity for metazoa from the spread of cancer to the thoracic region.
Intravenous pyelogram. After injecting a contrast agent into a vein, the urinary system is examined using an X-ray. This test can pick up abnormal parts of the urinary tract caused by the spread of cancer.
Other investigative methods include CT (computed tomography), which is a three-dimensional X-ray that can detect the extent of the cancer and can be used in place of chest X-ray and intravenous pyelogram.
MRI - Magnetic resonance imaging uses magnetic fields and radio waves to create a detailed image inside the body. It is used to detect the size and spread of a tumor with high accuracy.
PET - positron emission tomography uses a radioactive substance injected directly into a vein, areas of the body with more active cells than normal are imaged. This examination is of great importance for detecting the spread of cancer to the lymph nodes.
Course
HPV infection attacks the cells in which the viral DNA is implanted. The infected cell then starts to produce proteins that are encoded by the viral DNA. These secreted proteins subsequently produce changes and malignancy in the affected tissues.
However, this progression occurs only if the human organism does not recognize the infection in time and is unable to eliminate it, i.e. interrupt it in a natural way.
A healthy body with sufficient immunity can eliminate such cells, producing antibodies once the virus is recognised, which means that not every woman infected with HPV will get cervical cancer.
Some women don't even know they have been infected because their body has produced antibodies and the woman has spontaneously recovered on her own.
However, once the infection is overcome after natural recovery, antibody levels and immunity are reduced, which can then reappear even after natural recovery, leading to reinfection, i.e. re-infection with the virus.
If a cell is infected with HPV, its DNA is incorporated into the cell.
There are two types of HPV
LR-HPV, or Low-Risk Human Papillomavirus, causes tissue changes such as papillomas (lump-shaped skin growths) or condylomas (skin growths, warts in the intimate area).
HRHPV, or High-Risk Human Papillomavirus, leads to malignant tissue changes.
Epidermoid carcinoma of the cervix develops slowly, with dysplasia, or tissue change, occurring first. Such changes can take place over several decades.
Advanced cervical cancer is manifested by abnormal vaginal bleeding, pain in the pelvic area, discharge from the vagina, pain during sex.
Fertility preservation
To preserve the fertility of a woman of childbearing age, it is possible in stage 1, as long as the lymph nodes are not affected. Cancer-affected tissue from the cervix is removed, leaving the uterus intact.
Stage 2 is treated by conization, or radial trachelectomy, in which most of the cervix and upper part of the vagina are removed.
Higher stages may require chemotherapy before conization or trachelectomy.
Cervical cancer and pregnancy
As HPV, the virus that causes cervical cancer, is also one of the common viruses that 80% of women are infected with, such an infection may not affect the course of pregnancy.
HPV itself does not directly threaten the fetus, but cancer is different.
When confirming cancer in pregnancy, it is important to consider the stage of the cancer.
Cervical cancer occurs most often during pregnancy in the mildest, first stage.
The method of treatment in each case depends on the gestational age at the time of diagnosis, but also on the size of the spread of the tumour cells.
What is also important is what is preferred with regard to the preservation of pregnancy and fertility.
Cancer treatment during pregnancy can harm the developing fetus.
Depending on the stage of the cancer, treatment can be delayed and left until after the baby is born.
If a higher stage is detected and treatment is urgent, some types of chemotherapy are given, which can be given at the same time as medication during pregnancy.
Vaginal delivery is only possible in stage 1 cancer, but he is more inclined to deliver by caesarean section.
How it is treated: Cervical Cancer
Treatment of cervical cancer: conization chemotherapy and other methods.
World Cancer Report 2014. World Health Organization. 2014. pp. Chapter 5.12. ISBN 978-9283204299.
"Cervical Cancer Treatment (PDQ®)". National Cancer Institute. 14 March 2014.
Kumar V, Abbas AK, Fausto N, Mitchell RN (2007). Robbins Basic Pathology (8th ed.). Saunders Elsevier. pp. 718–721. ISBN 978-1-4160-2973-1.
Kufe D (2009). Holland-Frei cancer medicine (8th ed.). New York: McGraw-Hill Medical. p. 1299. ISBN 9781607950141.
Bosch FX, de Sanjosé S (2007). "The epidemiology of human papillomavirus infection and cervical cancer". Disease Markers. 23 (4): 213–227.
"Cervical Cancer Prevention (PDQ®)". National Cancer Institute.
"Human Papillomavirus (HPV) Vaccines". National Cancer Institute. 29 December 2011.
"Global Cancer Facts & Figures 3rd Edition" (PDF). 2015. p. 9.
Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, Bray F (May 2021). "Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries". CA: A Cancer Journal for Clinicians. 71 (3): 209–249.
"Defining Cancer". National Cancer Institute. 17 September 2007.
Yadav, Prakash Chand; Pandey, Shibendra Raj; Thapa, Ankit; Kishor Chaudhary, Deepak; Sah, Krishna Kumar (30 October 2021). "Updates on Cervical Cancer". North American Academic Research Journal.
Tarney CM, Han J (2014). "Postcoital bleeding: a review on etiology, diagnosis, and management". Obstetrics and Gynecology International. 2014: 192087.
Dunne EF, Park IU (December 2013). "HPV and HPV-associated diseases". Infectious Disease Clinics of North America. 27 (4): 765–778.
Ramachandran D, Dörk T (October 2021). "Genomic Risk Factors for Cervical Cancer". Cancers. 13 (20): 5137.
"FDA approves Gardasil 9 for prevention of certain cancers caused by five additional types of HPV". U.S. Food and Drug Administration. 10 December 2014.
Tran NP, Hung CF, Roden R, Wu TC (2014). Control of HPV infection and related cancer through vaccination. Recent Results in Cancer Research. Vol. 193. pp. 149–71.
World Health Organization (February 2014). "Fact sheet No. 297: Cancer".
"SEER Stat Fact Sheets: Cervix Uteri Cancer". NCI. National Cancer Institute. 10 November 2014.
World Cancer Report 2014. World Health Organization. 2014. pp. Chapter 1.1. ISBN 978-9283204299.
"Cervical cancer prevention and control saves lives in the Republic of Korea". World Health Organization. Retrieved 1 November 2018.
Canavan TP, Doshi NR (March 2000). "Cervical cancer". American Family Physician. 61 (5): 1369–1376.
I graduated from the Secondary Medical School in Nitra, which gave me the basis for a career in healthcare. After school I worked for three years in the surgical department and then in the department of Anaesthesia and Intensive Care Medicine. In addition to my employment, I completed my bachelor's degree at the Faculty of Health Care in Banská Bystrica in Nursing and completed my specialisation studies in Anaesthesiology and Intensive Care Medicine. Since my childhood I was determined to become a health professional and help people with their health problems. Continuous education and study of new professional topics related to health care, which is constantly evolving, and gaining practical experience, helps me to write professional articles for this portal, which is available to everyone. My hobbies are multifaceted, I am also involved in healthy nutrition, overall healthy lifestyle. I spend my free time on education, creative work, handicrafts in cooperation with my daughter, thanks to which, we do not know boredom.
. Photo: Getty Images.")